Has the case for radical NHS reform been made?
A major reason given by the coalition Government to justify the need for radical reform of the NHS is that the demands and expectations of an aging population combined with technological advances in medical care, and a financial crisis, mean that the current model is not sustainable financially.
The Government also claim the NHS performs badly compared to other nations in terms productivity and efficiency, as well as clinical outcomes.
On the former claim, Professor John Appleby, chief economist from the King’s Fund wrote an interesting data briefing for the BMJ, Can we afford the NHS in future? He noted Andrew Lansley’s comments to a Daily Telegraph article in June 2011:
“If things carry on unchanged, this would mean real terms health spending more than doubling to £230 billion (by 2030)......This is something we simply cannot afford.”
Appleby commented that this was a short step to an argument that the NHS must change (because unchanged equals unaffordable) and that the change it needs are the Secretary of State’s reforms i.e a version of the “politician’s syllogism”:
1. The NHS must change (otherwise it is unaffordable)
2. This (the reforms) is change
3. Therefore we must do this (the reforms).
Appleby went on to critique Lansley’s argument and concluded that “Spending on health will be a matter of choice, not affordability”
Professor Ian Greener’s recent blog also laid waste to the Government’s case for change and is essential reading. He noted that the Government approach to policy making is known as a ‘garbage can’ approach in the academic literature ie a solution in search of a problem- not evidence-based policy, but ideologically-driven policy.
Thus the Government are starting from a very weak position if they think radical change to the system is needed.
So what about the reforms themselves? Do they offer a solution to the fulfilling the long term future healthcare needs of our population, or not?
In my opinion, you only have to scratch the surface to see that the proposed NHS reforms will make things worse not better and this is the case from a professional, organisational and economic perspective.
Professional perspectives and effects of the reforms
From a clinical viewpoint, all professional bodies have concerns that the reforms will damage the NHS, fragment care, reduce access to care, increase inequalities, and undermine medical professionalism and the doctor patient relationship. In fact these concerns have hardened more recently, and thus the majority of professional and representative bodies of healthcare professionals are now callinging for the bill to be withdrawn. It therefore really makes you wonder how on earth MPs and Peers can even consider passing this legislation in the face of such professional opposition. The following remarkable statements from clinical leaders only serve to emphasise this:
Professor Lyndsey Davies, President of the UK Faculty of Public Health (UKFPH):
“It is clear that the majority of our members now believe that the Health and Social Care Bill, if passed, will damage the NHS and the health of people in England”
Dr Clare Gerada, Chair of the Royal College of GPs
“GPs don’t think the bill is going to create a patient led NHS, they don’t think it is going to increase autonomy, they don’t think it is going to improve patient care, and they don’t think it is going to improve healthcare inequalities”
Crucially, in terms of addressing the needs of an aging population, which is a key Government objective and a reason for reform, this statement from the British Geriatric Society calling for withdrawal of the bill (by it’s President Professor Finbarr C Martin) completely undermines the Government’s argument and credibility:
“It has become clear that the proposed legislation is both deeply flawed in detail and deeply troubling in its possible consequences. Our position is informed from the perspective of our members' knowledge and commitment to the health and community services needed by older people. We are concerned that the Bill does not support the changes necessary to provide integrated, high quality consistent care for our ageing population and has a serious risk of undermining the progress made in recent years”
He also states:
“The BGS remains committed to work in partnership with all health and social care services to ensure our ageing population receives the best care possible. In our view the provisions in this Bill will be a step backwards in attempts to do this”
Thus from a clinical professional perspective, the Government’s reforms will fail to do what they say on the tin.
Organisational perspectives and effects of the reforms
One of the key arguments the Government has put forward to justify the reforms is to cut bureaucracy and save money. However, several respected commentators have highlighted the fact that the bill increases bureaucracy and complexity of the system and will increase costs.
Professor David Colquhoun has explained this well in his blog and produced some really useful diagrams to show the complexity of the new system compared to the previous system.
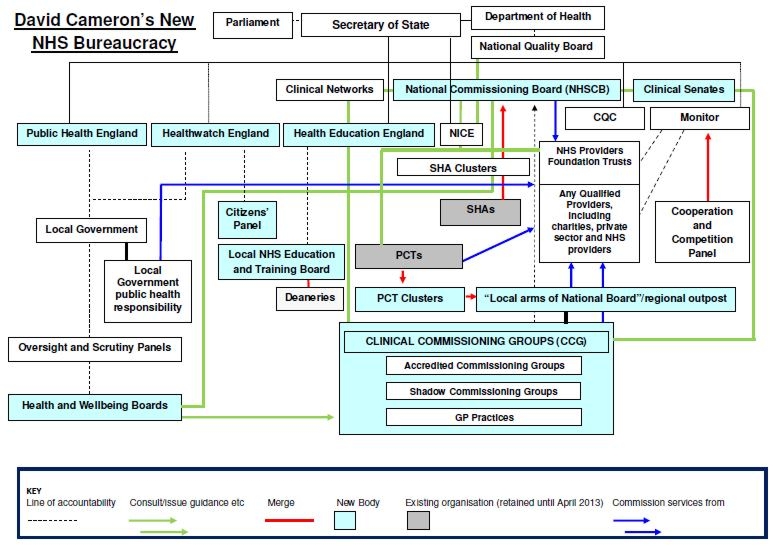{kind=link}
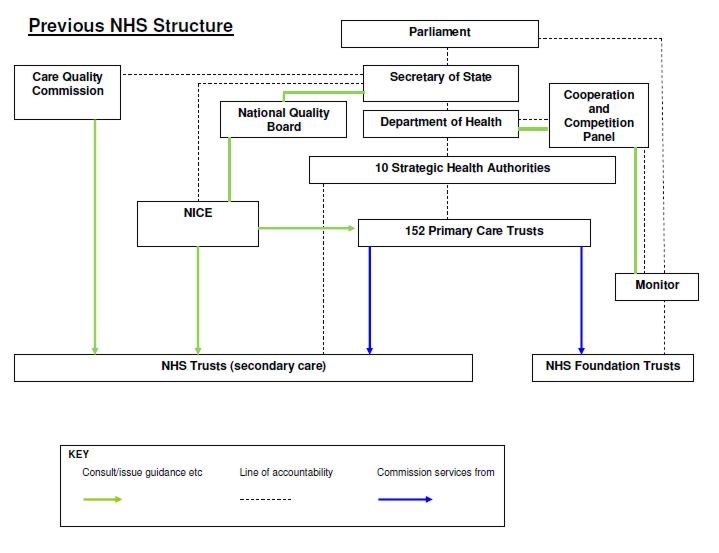{kind=link}
Roy Lilley has also explained how 3 layers of management have been replaced by 7 layers.
This is clearly a major reorganising and restructuring task and the Government estimates of these costs have been challenged by academics including Professor Kieren Walshe from the Manchester Business School and Professor Patrick Dunleavey from the LSE
Current estimates of the reorganisations are around £4 billion compared the Government figure of £1.3 billion.
Walshe states that “Little of the current architecture of the NHS will survive these changes unscathed.”
He then offers this advice to the Government:
“In brief, the government should learn three things from the history of NHS reorganisation:
1.Firstly, structural reorganisations don’t work.
2.“reorganisation adversely affects service performance
3. the transitional costs of large scale NHS reorganisations are huge”
Patrick Dunleavey states that the reforms have all the hallmarks of a “policy fiasco”.
Thus from an organisational perspective, the Government’s reforms fail to do what they say on the tin.
Market based systems and financial perspectives and effects of the reforms
For the NHS market to function there needs to be patient choice to drive competition between a plurality of Any Qualified Providers (AQP). Money then follows the patient through payment by results (PbR).
Stimulating competition and patient choice is one of the key aims of the bill. Andrew Lansley made what is now an infamous speech to the NHS confederation in 2005, where he stated that:
“The first guiding principle is this: maximise competition.... which is the primary objective”.
“Competition and choice are not just slogans. They are a policy whose time has come.”
He went on to describe how this would be achieved - by maximising the numbers of purchasers and providers in the system.
His method of increasing numbers of purchasers is by getting money closer to the patient (consumer) ie to GPs or patients themselves:
“The statutory formula should make clear that choice should be exercised by patients, or as close to the patient as possible, thereby maximising the number of purchasers and enhancing the prospects of competition, innovation and responsiveness to patients”
This is why his reforms are placing £60 billion of the NHS budget in the hands of “GP led” Clinical Commissioning Groups and why the policy of patient held budgets is being expanded.
In terms of maximising the numbers of providers, this will be achieved through the Any Qualified Provider (AQP) policy, where private companies and third sector (non profit) organisations are encouraged to enter the new market.
This creation of excess capacity in the system is the only way for patient choice and the market to function, which is confirmed by Lansley himself:
“The reforms I describe are designed to stimulate a significant capacity response”
However, having excess capacity is inherently inefficient, especially in a single payer system where there is a finite amount of money. Also very worrying is the drive to promote citizen–consumerism in healthcare, where patients act like consumers in a marketplace and shop around for health services. This is a system that responds to wants rather than needs, and is a recipe for inflating healthcare expenditure and creating inefficiencies through overtreatment and undertreatment.
So the slogan “No decision about me without me” is really about the idea of citizen- consumerism and increasing consumer power in the new healthcare market.
This clearly has highly significant cost implications for a single payer system.
If we now factor in the transaction costs of the market, it becomes apparent that it is highly unlikely that the single payer system can survive. This important paper in the BMJ, shows how the market has inflated costs in the US system. Moreover, in the UK, research from Karen Bloor of York University, which was cited by the Health Select Committee’s report on Commissioning in 2009, has estimated that administrative costs of the NHS following the introduction of the internal market reached about 15% of total NHS budget versus ~5% prior to the purchaser-provider split. The new market may reach higher percentages as the number of market transactions will increase and the need for private commissioning support through the Framework for External Support for Commissioning (FESC) is encouraged.
Thus from a financial perspective, the Government’s reforms will fail to do what they say on the tin.
In fact the reforms will. Coupled with increased costs associated with the reforms, the system will break under the pressure.
Future perspectives and effects of the reforms on creating a mixed funding system
The new market system will increase healthcare expenditure and force the NHS into financial meltdown. This will be catalysed by the McKinsey £20 billion QIPP efficiency drive, which amounts to a 4% per year efficiency saving until 2015. This scale of savings has not been attempted in any healthcare system in the world and it will lead to the demise of the single payer system, which Derek Wanless concluded was the most cost efficient way to fund the NHS. This then opens the door to a mixed funding system with increasing use of private insurance, user fees and top up payments.
And this is where we come to the heart of it - the reforms will makes this transition happen in the following ways:
• Firstly, Clinical commissioning groups will increasingly becoming rationing bodies, driving up waiting lists and reducing the number of NHS core services. Thus there will be an increasing demand for healthcare insurance as waiting lists go up. The QIPP efficiency measures will act as a catalyst to this process;
• Secondly, Foundation Trusts can borrow money from the City to invest. They will have to repay this by treating more NHS patients and more private patients. This will be aided by the raising the cap on private patients’ income for FTs to 49%. However, financial pressures will drive foundation Trusts into further debt burdens forcing closures, mergers and private management takeovers. This is already happening. In fact, this whole process is crucial to stimulating the private healthcare insurance and private provider industry.• Thirdly, there will be a new insurance market set up for top ups and co-payments; and
• Fourthly, in the next Parliament, it is likely that more direct patient charges will be introduced.
A failure of the NHS to provide a comprehensive service and the move towards opening up a mixed funding system requires the Secretary of State to abdicate his/her duties and powers to provide a comprehensive healthcare service to the nation’s population. This effectively denationalises the NHS and explains why the Government will not back down on Clause 1 and related clauses, which have been hotly debated in the Lords. They need to abolish these clauses to abolish the NHS and create the mixed funding systems. The work of Peter Roderick, Allyson Pollock and others is an essential read to understand this in more detail. I therefore strongly recommend the Duty to Provide website.
English citizens will increasingly have to consider taking out healthcare insurance policies as financial pressures cause the NHS to fail. Healthcare rationing by CCGs, Rising waiting lists, and reduction in NHS core services will fuel the insurance industry’s engine. This clearly has the most adverse effect on the most vulnerable in society because of the Inverse Care Law .
Finally, opening up the NHS to EU competition law will dramatically increase the amount of capital available to bring into our health service, but ultimately this capital will flow back to the investors at a profit, which will be at the expense of the UK citizens as taxpayers and in the form of private healthcare insurance premiums and out of pocket healthcare expenditure.
Conclusion: The politics and false economy of the reforms
The Government’s reasons for radical reform of the NHS are flawed, lacking in evidence, and driven by ideology. Their solutions will actually create more problems by increasing healthcare costs and bankrupting the NHS, leading to a mixed funding system of healthcare, with increasing marketisation and privatisation. Of course, increasing privatisation is a key supply side economic policy of the Government, which they are applying right across the public sector. New Labour were doing similar things, but not in such a drastic manner. I have discussed the politics of this neoliberal approach in another blog. The basic premise is that privatisation of public services will reduce the tax burden on corporations, reduce inflation and stimulate economic growth. However, the drive towards privatisation and a mixed funding system will increase economic and healthcare inequalities, which are both known to damage economic growth, which in turn impacts heavily upon the social determinants of health, causing a viscous circle of greater inequality. This is in direct contradiction to Clause 3 – the new duty of the Secretary of State for Health to reduce health inequalities.
The reforms will be economically damaging for a number of reasons. Citizens will have less money in their pockets as they have to pay for increasing proportions of their healthcare costs. Thus they will have less money to spend in their local economies. In addition, private companies will reduce terms and conditions for health workers who will have less money to spend in their local economies. These companies will also siphon off taxpayers money into their profit margins, the meteoric pay packets of their CEOs, and offshore tax havens. This will all be damaging the UK economy and thus NHS privatisation is a false economy.
We are about to lose our greatest institution, which is a highly performing and popular healthcare system. The NHS not only delivers on access, equity and fairness, but also acts to redistribute wealth around the country and stimulate local economies through the multiplier effect, helping local private businesses to grow and help stimulate the overall economy. Let’s not lose it to an ideologically driven coalition government, who have absolutely no democratic mandate to dismantle it.
You state : 'Derek Wanless concluded was the most efficient way to fund the NHS'.
ReplyDeleteIs he any relation to the Derek Wanless who was the former head of risk at Northern Rock Bank ? The latter Derek Wanless was severely castigated for his recklessness, imprudence, and lack of prescience, by the Treasury Select Committee, when investigating the multi-billion pound failure at Northern Rock. Wanless was deemed culpable in the bank's demise.
http://www.youtube.com/watch?v=fgsTid97h6g
It is a bit rich that we should be indulged with the wisdom of Wanless on the NHS, when we will be paying for his costly lack of judgment as a banker for decades to come, and that was supposedly his core discipline.
The moral of the Curate's Egg comes to mind. The callow curate had to be reminded by the wise old bishop that if an egg is part tainted, then it is fair to assume that is all tainted !